When gabapentin and pregabalin were first approved for epilepsy, few expected they’d become go-to treatments for nerve pain. Today, they’re among the most prescribed drugs for conditions like diabetic neuropathy, post-shingles pain, and fibromyalgia. But with rising use comes rising risk. Gabapentinoid safety isn’t just about whether the drug works-it’s about whether it’s being used safely, at the right dose, and with proper monitoring.
How Gabapentinoids Are Dosed-And Why It Matters
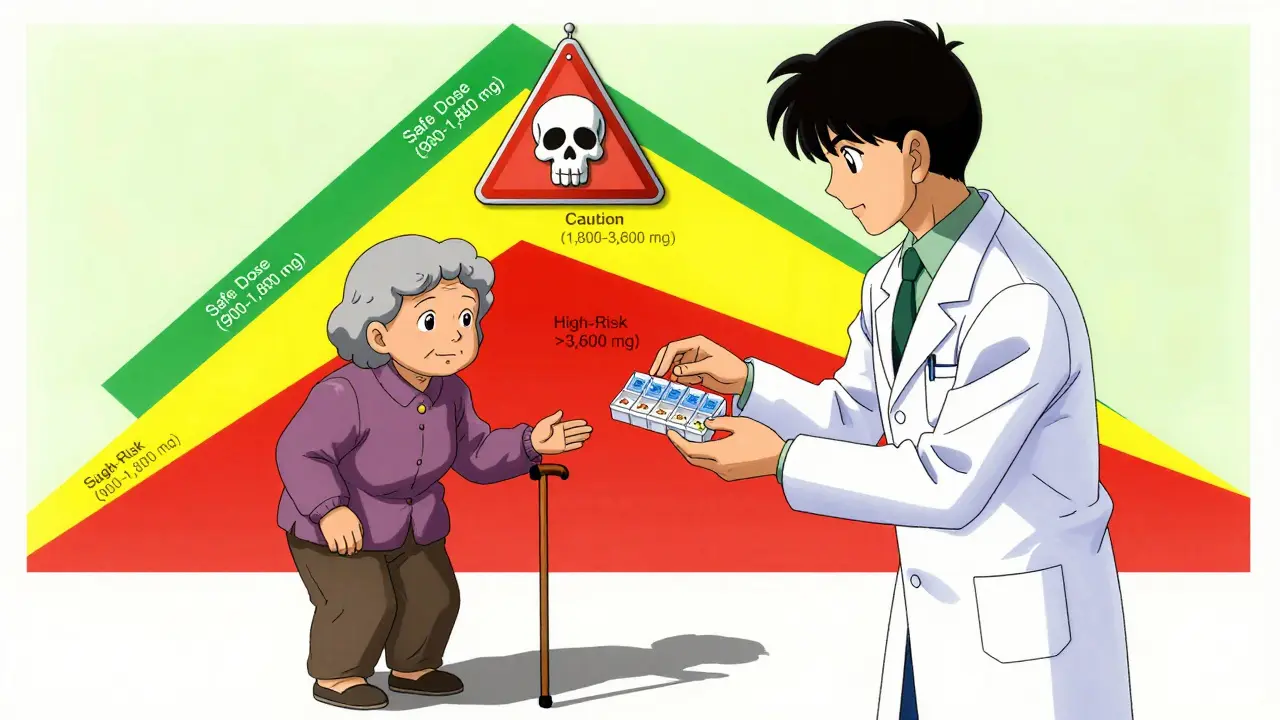
Dosing gabapentinoids isn’t one-size-fits-all. It’s not like taking an aspirin. Start too high, and you’re asking for trouble. Start too low, and you might not get relief. The key is patience.For gabapentin, most doctors begin at 300 mg once a day. After a few days, they’ll bump it to 300 mg twice daily, then three times daily. The goal isn’t to max out-it’s to find the lowest dose that eases pain. Many patients see improvement at 900-1,800 mg daily. Pushing beyond 1,800 mg rarely adds more pain relief but nearly doubles the chance of dizziness and falls, especially in older adults.
Pregabalin follows a similar pattern: start at 75 mg twice daily, then increase to 150 mg twice daily after a week. The maximum is 600 mg daily. But here’s the catch: studies show that doses above 300 mg twice daily don’t help more pain, just more side effects.
Renal function changes everything. If your kidneys aren’t working well, your body can’t clear these drugs. That means they build up. For someone with a creatinine clearance under 30 mL/min, the maximum gabapentin dose drops to 900 mg daily-or even lower. Many providers skip this check. Don’t. Always get a kidney test before starting.
Dizziness: The Silent Threat
Dizziness isn’t just annoying-it’s dangerous. One in five people on gabapentinoids reports dizziness. For those over 65, that number jumps to 40%. And it’s not just about feeling off-balance. Dizziness increases fall risk, which can mean broken hips, hospital stays, or even death in older adults.The worst part? Dizziness usually hits in the first week, right when people are ramping up their dose. A 2021 study found 68% of dizziness cases occurred during dose increases. That’s why slow titration saves lives. Instead of increasing every 2-3 days, stretch it out to 5-7 days. If you’re 70 or older, start at 100 mg daily and creep up by 100 mg per week.
Evening doses make morning dizziness worse. If you take your last dose at 8 p.m., you’re likely to wake up feeling foggy. Switching to morning and afternoon doses can cut dizziness by half. And if you’re already dizzy? Don’t wait for your doctor to ask. Speak up. A 2023 analysis of patient reviews found that 41% quit gabapentin because of dizziness-but 73% of those on 900-1,800 mg daily said side effects were manageable.
Misuse Is Real-And Getting Worse
Gabapentinoids aren’t opioids, but they’re being used like them. People with opioid use disorder are increasingly mixing gabapentin with heroin or fentanyl to boost the high or ease withdrawal. The CDC found a 497% spike in gabapentin-related overdose deaths between 2012 and 2020. In 2021, over 15 million Americans misused prescription pain relievers containing gabapentin.Why does this happen? At doses over 3,600 mg daily, some users report euphoria, relaxation, or a “floaty” feeling. On forums like Reddit, users openly share how they’ve cranked their dose to 4,800 mg daily to get that effect. That’s not treatment-that’s abuse. And it’s deadly. Emergency room visits tied to gabapentin misuse have doubled since 2018.
Doctors are catching on. As of 2023, 49 U.S. states now track gabapentin in prescription monitoring programs. The FDA added misuse warnings to labels in 2019. The American Society of Addiction Medicine now recommends screening every patient for substance use before prescribing. Urine drug tests aren’t optional-they’re necessary.
Who Should Avoid Gabapentinoids?
Not everyone should take these drugs. If you’re over 70, especially if you’re frail or have balance issues, the risks often outweigh the benefits. Studies show most elderly patients get relief at just 900 mg daily-and that’s enough. Higher doses don’t help more, they just make you fall more.People with a history of substance use disorder should avoid gabapentinoids unless no other option exists. Even then, they need close supervision: weekly check-ins, random urine screens, and a clear plan to taper off if misuse shows up.
And if you’re pregnant? Data is limited. While gabapentin isn’t known to cause birth defects, it does cross the placenta. Talk to your doctor. Don’t assume it’s safe just because it’s not an opioid.
What Safe Prescribing Looks Like
The best practices aren’t complicated. They’re just often ignored.- Start low: 100-300 mg daily for pain, especially in older adults.
- Go slow: Increase by no more than 300 mg every 5-7 days.
- Check kidneys: Get a creatinine clearance test before starting and every 3-6 months.
- Watch for dizziness: Ask patients weekly. Use a simple question: “Have you felt unsteady or lightheaded since your last visit?”
- Limit supply: For new prescriptions, give no more than a 7-day supply. Reassess before refilling.
- Taper properly: Don’t stop suddenly. Cut dose by 300 mg every 3 days over at least a week to avoid withdrawal seizures.
Some clinics now use the START protocol: Screen for kidney function and substance use, Titrate slowly, Assess dizziness weekly, Review necessity monthly, and Taper appropriately. It’s simple. It works.
The Future: Safer Prescribing, Safer Drugs
Prescriptions for gabapentinoids dropped 8.7% in 2022-the first decline in 20 years. Why? Because providers are finally listening. The FDA updated labels in 2023 to highlight fall risks in seniors. The CDC now labels doses over 1,800 mg daily as “high-risk.” Pharmaceutical companies are testing abuse-deterrent versions-like extended-release pills that can’t be crushed or injected.But the real change isn’t in the pills. It’s in the practice. Safe prescribing means asking: Is this the lowest dose that works? Is the patient at risk for falls? Do they have a history of substance use? If the answer is yes to any of those, it’s time to reconsider.
Can gabapentin cause addiction?
Gabapentin and pregabalin aren’t addictive in the same way as opioids, but they can be misused. Some people take high doses to feel euphoric or to enhance the effects of other drugs like alcohol or opioids. The FDA added misuse warnings to labels in 2019, and the CDC reports a sharp rise in overdose deaths involving gabapentin. Risk is highest in people with a history of substance use disorder.
Why does gabapentin make me dizzy?
Gabapentinoids affect brain chemicals involved in balance and coordination. Dizziness occurs in 20-30% of users and is dose-dependent. Higher doses-especially above 1,800 mg daily-double the risk. It’s most common in the first week of treatment, during dose increases. Older adults and those with inner ear issues are at highest risk.
Is 1,200 mg of gabapentin too much?
For most people with nerve pain, 1,200 mg daily is within the recommended range. It’s often effective and carries a lower risk of dizziness than higher doses. Many patients find relief between 900-1,800 mg daily. Doses above 1,800 mg rarely improve pain further but significantly increase side effects.
How long does it take for gabapentin to cause dizziness?
Dizziness usually starts within the first week, especially during dose increases. Studies show 68% of cases occur during the titration phase. It’s less common after the body adjusts, but it can return if the dose is raised too quickly or if another medication is added. If dizziness appears after weeks of stable dosing, check for new interactions or worsening kidney function.
Can I stop gabapentin cold turkey?
No. Stopping suddenly can cause withdrawal symptoms like anxiety, insomnia, nausea, and even seizures. The FDA recommends reducing the dose by 300 mg every 3 days over at least a week. For long-term users, tapering over 2-4 weeks is safer. Always consult your doctor before stopping.
Next Steps: What to Do If You’re Taking Gabapentinoids
If you’re on gabapentin or pregabalin:- Know your dose. Is it above 1,800 mg daily? Ask your doctor if you can lower it.
- Track dizziness. Keep a simple log: “Did I feel off-balance today?” Share it at your next visit.
- Get your kidney function checked. A simple blood test takes minutes.
- Be honest about substance use. Your doctor needs to know if you’ve used alcohol, opioids, or other drugs.
- Don’t take more than prescribed. Even if you think it helps more, it might be making you unsafe.
If you’re a prescriber: use the START protocol. Screen, titrate slowly, assess weekly, review monthly, taper properly. It’s not extra work-it’s better care.
Gabapentinoids can help. But they’re not harmless. Safety isn’t about avoiding them-it’s about using them wisely.
Aisling Maguire
February 27, 2026 AT 23:28Also, if you're scared of side effects, maybe don't start at 1800mg on day one. Just saying.
Katherine Farmer
March 1, 2026 AT 21:48Brandie Bradshaw
March 2, 2026 AT 00:55And yet, we're told to 'start low, go slow' as if that's a breakthrough. It's basic physiology. Why is this even a conversation?
bill cook
March 3, 2026 AT 17:56Noah Cline
March 3, 2026 AT 23:07Yet, 68% of primary care providers still fail to order baseline creatinine. That's not negligence - it's systemic failure.
Lisa Fremder
March 4, 2026 AT 14:11Justin Ransburg
March 6, 2026 AT 13:28Let's stop treating patients like numbers. Let's start treating them like people.
Sumit Mohan Saxena
March 8, 2026 AT 00:20Brandon Vasquez
March 9, 2026 AT 11:37She didn't know it was dangerous. Her husband didn't know either. This isn't about blame. It's about education. We need to talk about this - not just in clinics, but in homes.
Vikas Meshram
March 9, 2026 AT 21:15And yes - I have documented patients who escalated to 4800mg daily to achieve euphoric effects. This is not 'misuse.' This is addiction. The terminology matters.